

A Comparison Study of HIFEM technology used in Emsella Treatments
MUCH IS ASKED ABOUT THE ACTUAL EFFECTIVENESS AND RESULTS OF EMSELLA, WHAT WE ALL WANT TO KNOW IS ‘DOES EMSELLA REALLY WORK? WHERE ARE THE STUDIES?’
As a relatively new technology and treatment option to treat incontinence by strengthening the pelvic floor muscles and reducing the vagina circumference, Emsella has alot to prove, especially given the high cost compared to other treatment options.
We thought we would delve into the technology behind it, High-intensity Focused Electromagnetic or HIFEM, patented by the innovators behind Emsella and used across the suite of ‘Em’ products including Emsculpt, Emface and Emsella, all providing muscle toning benefits to the body.
WHAT IS HIFEM TECHNOLOGY?
High-intensity focused electromagnetic (HIFEM) technology is a powerful, non-invasive treatment that uses electromagnetic energy to build muscle and burn fat. It works by stimulating muscle contractions in a similar way to exercise, but with a much higher intensity, reaching much further into the muscle fibres, and in the case of Emsella, targets deep into the complex network of pelvic floor muscles.
The alternative to HIFEM, EMS uses electrical pulses to mimic nerves and stimulate the top layers of the muscle. It can help to tone and firm muscles, but the results aren’t as effective or as permanent compared to HIFEM. EMS is also unable to burn fat, so the outcome is much less ideal for results and value. There are many EMS chairs on the market offering the same outcomes as HIFEM, however, it is not possible given EMS will not work as effectively on ‘cold’ muscle as HIFEM.
In our research, we found a great scientific study that provides conclusions with data and visuals that HIFEM and Emsella is recommended to treat incontinence. The study was done on 95 women who have undergone childbirth in the last 6 months, an ideal cohort for Emsella treatments. We have converted the study into laymans terms for the benefit of this blog, however, have not altered any of the figures or exagerated the language used.
A STUDY COMPARING THE EFFECTS OF HIGH-INTENSITY ELECTROMAGNETIC (HIFEM) THERAPY AND ELECTROSTIMULATION FOR TREATING WEAK PELVIC FLOOR MUSCLES AND URINARY INCONTINENCE IN WOMEN
Elena Silantyeva, MD, PhD,∗ Dragana Zarkovic, MSc,† Evgeniia Astafeva, MD,∗ Ramina Soldatskaia, MD,∗ Mekan Orazov, MD, PhD,‡ Marina Belkovskaya, MD, PhD,∗ and Mark Kurtser, MD, PhD∗, Academician of the Russian Academy of Sciences
OBJECTIVES:
Pelvic floor muscles (PFMs) weakening and urinary incontinence (UI) represent health issues that have a negative impact on daily life. This study compares the immediate efficiency of high-intensity focused electromagnetic (HIFEM) therapy with BTL EMSELLA and electrostimulation with BioBravo for the treatment of weakened PFMs, accompanied by the UI.
METHODS:
Ninety-five parous women were considered for the study. Symptomatic patients received either HIFEM (Group I), or electrostimulation (Group II) treatment. Treated patients completed 10 therapies scheduled 2 to 3 times per week (HIFEM) or every other day (electrostimulation). Patients underwent examination by 3-dimensional transperineal ultrasound at the baseline and post treatments. Levator-urethra gap, anteroposterior diameter, laterolateral diameter of levator hiatus, and hiatal area were measured. In addition, Pelvic Floor Disability Index 20 questionnaire and subjective evaluation of patient’s intimate health were assessed.
INCLUSION CRITERIA AND ETHICS:
From 2018 to early 2019, 95 women who had given birth and were of reproductive age were referred to Hospital Lapino for this study. The study is based on data collected from these women during their pre- and post-treatment exams.
To participate, women had to be between 18 and 45 years old and have had a vaginal delivery at least 6 months prior. Women were excluded if they had conditions like pelvic organ prolapse, were pregnant (verified by a pregnancy test), or had metal implants in the lower back, pelvis, or hips. Women with pacemakers, other electronic devices, or contraindications for physiotherapy were also excluded. All participants provided informed consent.
TREATMENT PROTOCOL:
Women who had weak pelvic floor muscles (PFMs) and urinary incontinence were treated with either the BTL EMSELLA device or the BioBravo device.
Group I – BTL EMSELLA uses high-intensity focused electromagnetic (HIFEM) technology to strengthen PFMs and reduce urinary incontinence. During treatment, patients sat fully clothed on a special chair that delivered magnetic pulses to the pelvic area. Each session lasted 28 minutes, and patients had 10 sessions, 2-3 times per week.

Group II – BioBravo is a portable, low-frequency stimulator used at home to treat urinary or fecal incontinence. After initial training, patients used the BioBravo device for 28-minute sessions, 3 times a week or every other day, completing 10 sessions in total.

EVALUATION OF RESULTS:
To track progress, various methods were used. During the first visit, patients underwent a medical history review, a gynecological exam, and a 3D ultrasound of the pelvic floor. Specific measurements like the size of the pelvic opening were taken. The ultrasound was repeated after treatment.
Patients also filled out the Pelvic Floor Disability Index 20 (PFDI-20) questionnaire to assess their pelvic muscle function and continence issues. Additionally, they answered “yes” or “no” to questions about their intimate health, including whether they experienced vaginal looseness, changes in vaginal shape, or urinary leakage during physical activities.
Safety and patient comfort were closely monitored, with patients reporting any side effects like pain, muscle fatigue, or bruising. Those using the BioBravo device at home were instructed to record any issues caused by the electrotherapy.
The study had a large enough sample size for proper statistical analysis, which was performed using specialized software.
RESULTS:
All 95 women were included in the study. Of these, 75 had weak pelvic floor muscles and incontinence issues. These women were divided into two groups:
Group I: 50 women (average age 31.1 years) received treatment with the EMSELLA device.
Group II: 25 women (average age 32.0 years) used the BioBravo stimulator.
Group III: The remaining 20 women (average age 27.2 years), who were healthy, served as a control group for the ultrasound measurements.
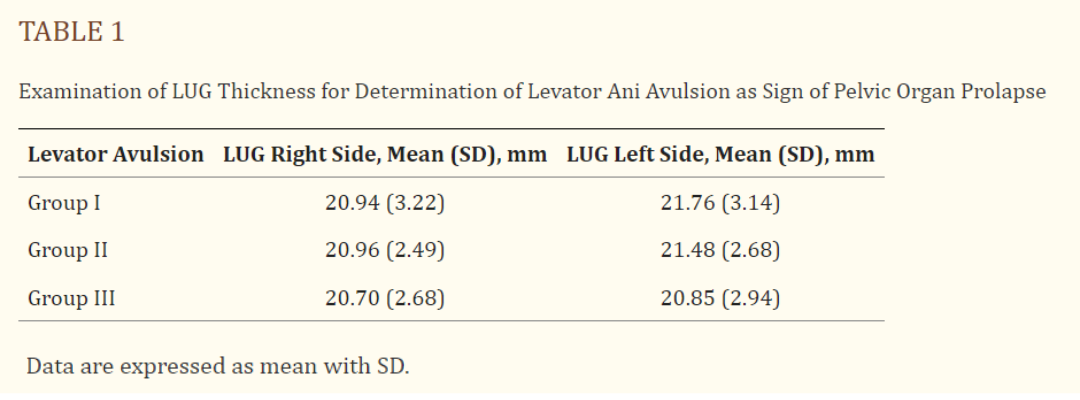
All participants completed their treatments without any negative side effects or pain. None of the patients experienced pelvic organ prolapse, and all met the criteria for the study. Minor differences in pelvic muscle thickness were not significant between groups.
3D ULTRASOUNDS OF THE PELVIC FLOOR:
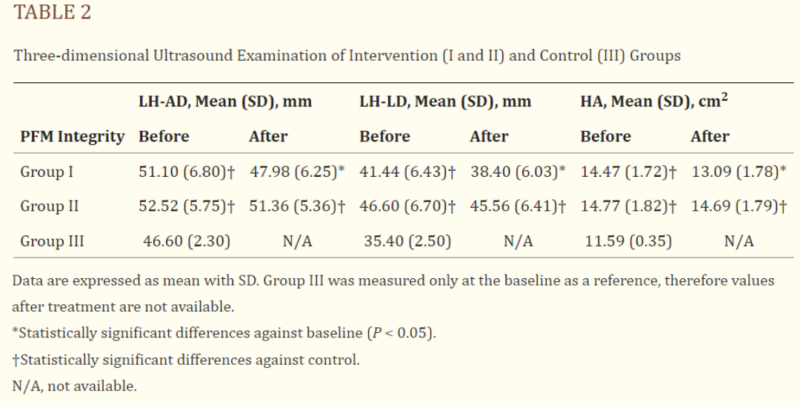
The results from the 3D ultrasounds are shown in Table 2. Before treatment, the patients in both treatment groups had significantly higher values in all pelvic floor measurements compared to the healthy control group. After the final therapy session, group I (who received HIFEM treatment) showed a significant reduction in these measurements (P < 0.05), bringing their values closer to those of the control group. Group II (who received electrostimulation) showed a similar trend, but the changes were not statistically significant (P > 0.05). This suggests that HIFEM technology had a more noticeable impact on improving pelvic floor measurements.
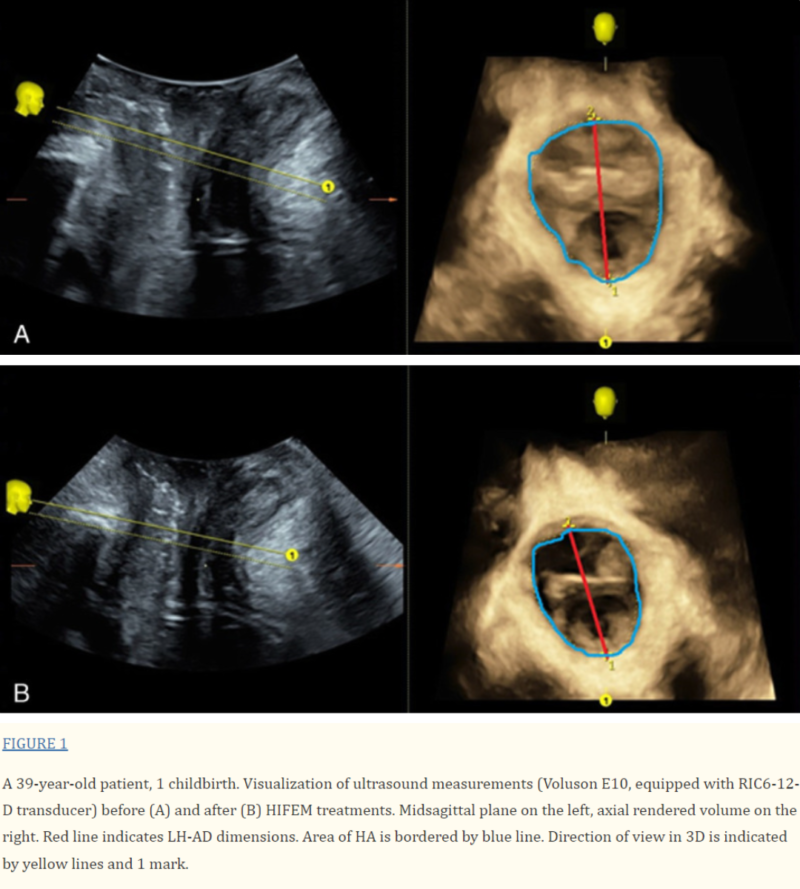
The 3D ultrasound images taken before and after HIFEM treatments are shown in Figure 1. It clearly shows improvements in the pelvic floor measurements, specifically in the LH-AD and HA parameters. The LH-AD thickness decreased by 2.6 mm, which is similar to the average reduction for all of group I (3.12 mm). Additionally, the HA measurement showed an even greater reduction of 1.83 cm², which is almost 0.5 cm² more than the group I average decrease of 1.38 cm².
PFDI-20 STANDARDISED QUESTIONNAIRE:
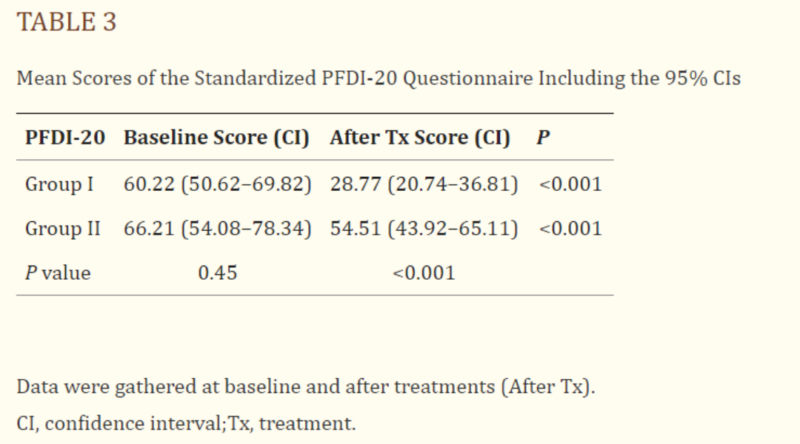
There was no significant difference in the initial PFDI-20 scores between the two groups, even though group II’s baseline score was slightly higher (P = 0.45). However, group I showed much greater improvement. After HIFEM treatments, patients in group I improved by an average of 31.45 points (52%, P < 0.001). Group II also improved but to a lesser extent, with an average increase of 11.70 points (18%, P < 0.001). When comparing the final scores after treatment, group I’s results were significantly better than group II’s (P < 0.001).
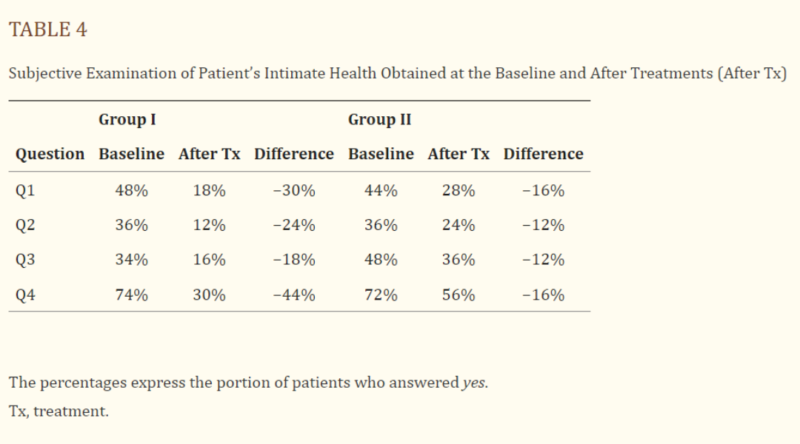
PATIENT’S SELF-EVALUATION:
The results of patients’ self-evaluations are shown in Table 4. The percentages represent how many patients answered “yes” to questions Q1 through Q4 about their symptoms. After treatment, both groups saw a decrease in the number of positive answers, but group I (HIFEM) showed much greater improvement compared to group II. On average, patients in group I reported twice as much improvement as those in group II. Notably, the biggest improvements in group I were seen in Q1 (vaginal laxity) and Q4 (urinary incontinence), with differences of up to 30% (Q1) and 44% (Q4), while group II only showed a 16% improvement.
SAMPLE SIZE AND POWER VERIFICATION:
Using a software tool called G-power, we determined that at least 16 patients were needed to find meaningful results in the data. This applies to both types of statistical tests we used (with a confidence level of 95% and effect size of 1). After analyzing the data, we double-checked the strength of our analysis and found that it had a power of 99%, meaning the results are very reliable.
DISCUSSION:
Based on the results, we found that HIFEM therapy is more effective than electrostimulation for treating weak pelvic floor muscles in the short term. Both subjective measures (patient surveys) and objective measures (3D ultrasounds) showed that HIFEM therapy led to greater improvements in pelvic floor strength and urinary incontinence.
Ultrasounds are a reliable way to examine the pelvic area. Since the pelvic floor is made up of complex structures, a 2D image might not show everything clearly, so we used 3D imaging for a more detailed view. This technology can detect pelvic floor weakness even before the patient notices symptoms, helping doctors start treatment early. The 3D scans allow us to measure specific areas of the pelvic floor and assess how well it’s functioning.
In our study, the patients who received HIFEM treatment had significant improvements in pelvic floor strength, as seen in the ultrasound results. These changes were not as noticeable in the group that received electrostimulation.
The data shows that HIFEM treatment led to better pelvic floor muscle function, reduced urinary incontinence, and improved quality of life. Both treatments were effective, but HIFEM showed much stronger results. The questionnaire results confirmed this, as group I (HIFEM) improved 2.68 times more than group II (electrostimulation). Group I saw over a 50% improvement in their scores, while group II only had an 18% improvement.
Patients in group I also reported fewer incontinence issues and less vaginal laxity after HIFEM treatment, while group II saw only modest improvements in these areas. This suggests that HIFEM provides better results because it strengthens the pelvic floor more effectively.
For pelvic floor muscle strengthening, it’s important to have strong contractions with rest periods. HIFEM therapy works well because it uses a high-intensity electromagnetic field to deeply stimulate the pelvic muscles, causing uniform contractions. On the other hand, electrostimulation might not be as effective because it doesn’t penetrate as deeply, meaning less energy reaches the pelvic muscles.
While electrostimulation has shown positive effects in the past, it’s still unclear if it’s better than traditional exercises for pelvic floor strengthening.
Our study involved relatively young postpartum women, but we believe the findings could also apply to older women, especially those going through menopause, who may have more severe symptoms due to hormone changes.
While we focused on short-term results, other studies suggest that the benefits of pelvic floor stimulation could last up to a year. However, after this period, some patients might need maintenance sessions to keep the improvements.
Although this study was short-term, the results were clear: HIFEM is more effective than electrostimulation. Future research should look into how long these results last and when retreatment might be needed. we recommend HIFEM therapy as an effective treatment for pelvic floor weakness and urinary incontinence.
Future research has shown a maintenance program of two top sessions every 6 months is enough to maintain results, alongside a program of pelvic floor exercises at home.
If you would like to try Emsella, a The Springwell Clinic, we offer 15 minute taster sessions so you can feel the effectiveness for yourself. You can book your Emsella taster and consultation online here, by calling 01628 308060 or email hello@springwellcinic.co.uk.